BCIs connect your brain’s electrical signals to external devices so you can control a cursor, a robotic arm, or software without using your hands. Early research began in the 1970s at UCLA and now companies like Neuralink, Synchron, and Precision Neuroscience are moving from lab demos to human implants and pilot systems.
You’ll get a plain-English view of what these systems do, why they matter at work today, and how they turn thoughts into practical control. Expect to read about noninvasive headsets, partially invasive ECoG and endovascular options, and fully implanted microelectrode arrays.
Think of BCIs as another way to give and get information faster—helping accessibility, speeding communication, and enabling hands-free control in AR/VR and robotics. You’ll also learn practical steps to pilot devices, evaluate vendors, and prepare your company for data and safety needs.
Key Takeaways
- BCIs turn brain signals into real-world control for hands-free tasks and accessibility.
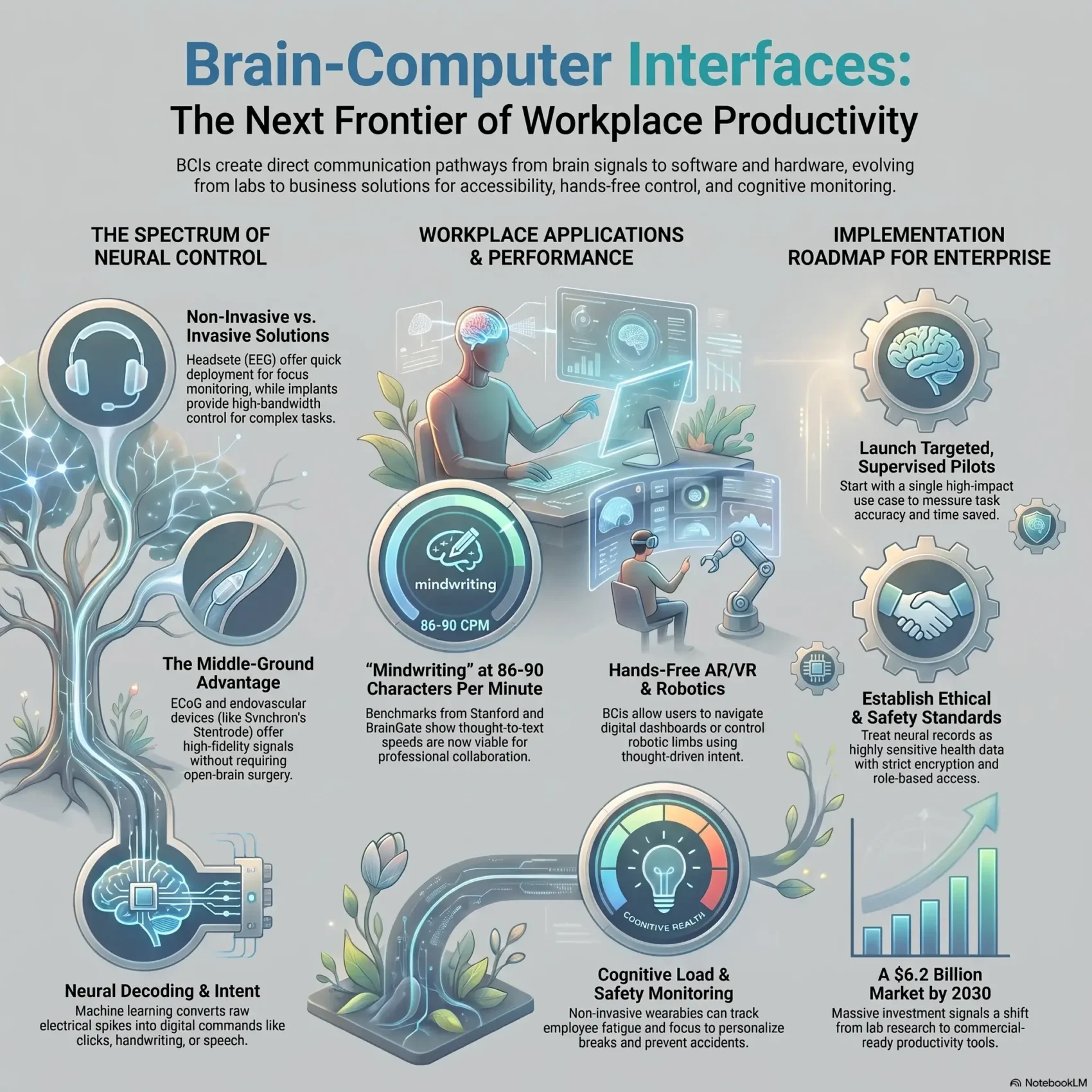
- Technology spans noninvasive headsets to implanted arrays; some vendors are in human trials.
- Early workplace wins include communication aids, task focus tools, and simple control flows.
- Plan pilots carefully and address data governance and safety from day one.
- Explore integration with existing systems and learn from vendors before wide rollout.
- For related work on emotion-aware systems that complement neural tools, see emotion AI at work.
What You Need to Know About brain-computer interfaces
Start here for a short, practical definition of devices that turn activity in the brain into digital commands and workplace value. A brain-computer interface creates a direct communication pathway between the brain’s electrical activity and external software or hardware.

Clear definition and why it matters
These systems capture neural signals and decode intent so you can control cursors, apps, or robotic tools without hands. That capability improves accessibility and can speed routine tasks in AR/VR, control rooms, and assistive workflows.
Quick primer on common terms
- BCI / BMI: abbreviations you’ll hear in vendor docs.
- Signals: electrical patterns the sensors record and the decoder translates.
- Electrodes: sensors on the scalp, on the cortex (ECoG), or implanted as microelectrodes.
“Closer sensors generally mean higher fidelity, but also more invasive methods.”
Practical takeaway: match device type to use case, plan data governance early, and expect learning curves as users and systems adapt.
From EEG to today: A brief history of BCIs
The story of modern neural control begins nearly a century ago, when researchers first captured brain rhythms and imagined new ways to use them.
Hans Berger, EEG, and Vidal’s challenge
In 1924 Hans Berger recorded human brain activity and identified alpha waves (8–13 Hz). That simple recording changed how people thought about measurable signals from the scalp.
In 1973 Jacques Vidal coined the term brain-computer interface and set a public challenge: use EEG to control external devices. Vidal’s work showed cursor control using visual evoked potentials and launched decades of research.
Key milestones in animal and human studies
Animal studies by Nicolelis, Donoghue, Schwartz, and Andersen in the 1990s–2000s proved monkeys could drive cursors and robotic arms from motor cortex activity. Those methods informed decoding of movement and intent.
- 2000s human implants moved the field from lab to patient impact.
- BrainGate enabled a paralyzed patient to control a robotic hand and cursor.
- Modern studies now focus on speech decoding, limb control, and stroke rehab.
“Funding from NSF, DARPA, and the BRAIN initiative accelerated development and real-world trials.”
How brain-computer interfaces work: Signals, decoding, and control
At the core of these systems is a simple chain: neurons produce electrical events, sensors capture those events as signals, and decoders convert them into control commands you can use.
Brain activity 101: Neurons, spikes, and local field potentials
Neurons fire tiny voltage spikes and create slower local field potentials. Those two activity types carry different information: spikes map closely to specific movement intent, while field potentials reflect broader state and rhythm.
Electrodes and sensors
Noninvasive tools like EEG and MEG measure scalp voltages or magnetic fields. fNIRS tracks blood flow with light. More direct options—ECoG on the cortex and microelectrode arrays in tissue—capture higher-fidelity signals.
Neural decoding and closed-loop control
Decoding uses machine learning to turn raw signals into intentions: cursor movement, handwriting, or speech. UCSF and Stanford demos show speech and handwriting decoding at usable speeds for patients.
Closed-loop systems add feedback and sometimes stimulation so models and users adapt over time. That improves accuracy, reduces fatigue, and helps a system stay aligned with changing brain signals.
“Good decoding needs clean signals, the right electrodes, and continuous adaptation.”
- Practical takeaway: match sensor fidelity to the control you need—higher fidelity means more precise movement or faster text entry.
- Plan sampling rates, channels, and data formats up front so integration with your IT systems is smoother.
Modalities compared: Non-invasive, invasive, and partially invasive
Compare the main ways people capture neural signals so you can match performance to real workplace needs.
Non-invasive headsets and wearables
EEG headsets are the easiest way to adopt this technology. You can deploy them quickly with minimal clinical setup.
They record scalp voltages, but those signals are weaker. That limits fine movement and high-speed text entry.
Invasive implants and microelectrode arrays
Implants sit in brain tissue and offer high-bandwidth control. That enables precise cursor and robotic movement.
Tradeoff: better signals require surgery, skull access, and careful recovery planning with clinicians.
Surface arrays (ECoG) and endovascular options
ECoG rests on the cortex under the skull and often hits a sweet spot: strong decoding without penetrating tissue.
Endovascular devices thread electrodes through blood vessels near motor areas, avoiding open-brain surgery.
- Quick deploy vs. high fidelity: headsets now, implants later.
- Surgical considerations: skull access, tissue involvement, recovery time, and safety.
- Operations: calibration, maintenance, and training differ by device and approach.
“Choose the method that matches your performance targets and risk tolerance.”
Leading BCI technologies and devices shaping the market
Below is a concise vendor-by-vendor snapshot to help you shortlist devices and match risk profiles to use cases.
Neuralink
Flexible-thread electrodes (1,024 channels) and a neurosurgical robot aim for high-channel recordings. The company received FDA approval for human trials in 2023 and has implanted multiple patients in its PRIME study.
Synchron
Stentrode uses an endovascular path via the jugular vein to reach vessels near motor cortex. That approach lowers surgical complexity and supports thought-driven clicks and typing; Synchron implanted the first U.S. patient in 2022 and partners with OpenAI and Nvidia.
Precision Neuroscience, Paradromics & Blackrock
- Precision Neuroscience: Layer 7 thin-film ECoG conforms to cortex and earned FDA 510(k) clearance in April 2025.
- Paradromics: Connexus uses 420 micro-needle electrodes for high-resolution signals; first human implantation occurred in May 2025.
- Blackrock: Pioneer of Utah arrays, driving high-channel research for speech restoration.
Neurable
Neurable builds consumer-grade EEG headphones (Enten, MW75 Neuro) focused on productivity, encryption, and analytics for everyday use.
“Match each device’s electrode strategy, channels, and placement to your decoding and IT needs.”
Workplace applications you can pilot today
Small, supervised pilots are the fastest way to test how thought-driven tools help real tasks. Start with clear goals: faster typing, reliable clicking, or device control. That keeps early projects low risk and focused on measurable value.
Hands-free computer control for accessibility and productivity
You can deploy noninvasive headsets to enable hands-free typing and clicking for employees with motor impairments or temporary injuries.
Studies from UCSF and Stanford show speech and handwriting decoding reach speeds that support real collaboration. Synchron demos thought-driven clicks for messaging and simple app control.
Communication aids: “Mindwriting,” spellers, and collaboration tools
Spellers and emerging mindwriting tools let non-verbal people send messages, manage social apps, and join chats. Pilot these as assistive services with clear privacy controls.
Human-robot interaction and smart environments
BCI systems already link to robotic arms, exoskeletons, and drones in research and DoD trials. You can test task-specific device control for repetitive handling or constrained-space operations.
Also try smart-environment pilots: adjust screens, lights, or AR/VR workflows by thought to reduce context switching and speed task flow.
- Design success metrics: click reliability, words-per-minute, task time, and user comfort.
- Plan IT needs: pairing, wireless management, and OS accessibility integration.
- Choose device type by use—headsets for quick pilots, clinical partnerships for high-fidelity device work.
“Run small pilots, measure simple metrics, and scale what improves access and productivity.”
BCIs for healthcare and rehabilitation at work
At work, neural tools are already helping patients relearn communication and regain basic control of devices they need for daily tasks.
Stroke recovery and spinal cord support: Clinical studies show real potential. UCSF’s ECoG work decodes intended speech, and Stanford has translated imagined handwriting into rapid text output. That progress helps people recovering from stroke or spinal cord injury use spellers, cursors, and robotic aids to resume job tasks.
Return-to-work pathways
You can build programs that pair clinicians, HR, and caregivers to align device choice, training schedules, and accommodations. Short, frequent sessions accelerate learning and reliable control.
Monitoring cognitive load and safety
Non-invasive headsets can track brain activity linked to fatigue and focus, letting you personalize breaks, rotate tasks, or enable assistive automation in safety-critical roles.
- Privacy-first data: require opt-in, strict role-based access, and occupational-health safeguards for any patient data.
- Success metrics: return-to-work milestones, communication speed, error rates, and user comfort.
- Device choice: use medical-grade systems when clinical control is needed; consumer wearables can inform workplace adjustments.
“Start small with clinical partners and scale what reliably improves access and performance.”
Implementing a BCI program: A practical roadmap for your company
Begin with a practical checklist that turns early curiosity into a testable pilot. A focused plan keeps costs down and shows whether a system adds real value for users and teams.
Pilot design: Use cases, stakeholders, and success metrics
Choose a single high-impact use to test. Pick willing participants and set measurable outcomes up front.
- Define the primary use and target metric (task accuracy, words per minute, or time saved).
- Map stakeholders: IT, accessibility, HR, legal, and facilities must know roles and timelines.
- Vet devices and vendors; prefer commercially supported options over research-only toolkits like BCI2000 unless you have engineering support.
“Performance improves with training and closed-loop feedback — plan your timeline accordingly.”
People, policies, and training: Change management for adoption
Size the pilot realistically. Plan daily session lengths, training cadence, and a clear support model.
Policies matter: set eligibility rules, voluntary participation, and accommodations from day one. Handle data governance and security approvals early to avoid delays.
- Create communication templates for participants and managers to build trust.
- Track metrics weekly and iterate your approach based on feedback.
- When targets are met, scale slowly to more sites or use cases without overextending teams.
Practical takeaway: treat pilot work as system development—short cycles, clear metrics, and vendor reliability win the day as you bring brain-driven tools into the workplace.
Data, privacy, and security: Safeguarding brain data
Before you launch a pilot, map what neural information flows through your systems and who can access it. Neural data includes electrical patterns that can reflect intended movement, speech, or cognitive state. Treat those recordings like health records: sensitive and regulated.
What neural data contains and why it’s sensitive
Neural signals can reveal intentions and fleeting thoughts. Non-invasive EEG, partially invasive ECoG (under the skull), and invasive arrays in brain tissue have rising sensitivity and risk. That changes retention policy, breach impact, and consent needs.
Encryption, governance, and U.S. compliance
Inventory data flows: on-device, in-transit, and at rest. Use strong encryption, key management, and role-based access. Log consent and audit trails so you can show who viewed information and why.
- Align pilots with HIPAA when occupational health or patients are involved.
- Vet vendors for secure update practices and incident response.
- Separate identifiers from signals to lower re-identification risk.
- Communicate clearly with employees about collection, usage, and retention.
“Treat neural records with the same controls you apply to clinical devices and protected health information.”
Safety, ethics, and equity in brain-computer interface deployments
Safety, ethics, and equal access should be the guardrails for any neural device program. You must set clear expectations for patients and people who will use these systems. That starts with plain-language consent and ends with long-term follow-up.
Informed consent and long-term device safety
Explain surgical risks—scarring, infection, and possible signal loss over time—for invasive options. Note that ECoG and endovascular approaches can reduce those risks.
Ensure patients know benefits, alternatives, and the plan for maintenance. Build monitoring, scheduled checkups, and rapid-response support into your approach.
Bias, accessibility, and protecting dignity
Design selection and training to avoid favoring only well-resourced users. Use fair recruitment, cover costs when possible, and design metrics that reflect diverse needs.
- Set an ethics review with clear exit and pause pathways.
- Provide caregiver training, maintenance plans, and fast support for device issues.
- Communicate risks and mitigations in everyday language to build trust.
“Prioritize human dignity and autonomy as you deploy any BCI in the workplace.”
Regulatory and reimbursement landscape in the United States
Before you buy or pilot any device, map the regulatory route and who will pay for surgery, upkeep, and upgrades. Regulation affects procurement timelines, liability, and the vendor evidence you need to review.
FDA pathways: Breakthrough Device, IDEs, and 510(k)
The FDA uses several paths that signal product maturity. Breakthrough Device status speeds review for high‑need therapies. Investigational Device Exemptions (IDE) allow clinical study in humans. A 510(k) clearance shows a device compares favorably to a legally marketed predicate.
Recent milestones matter for your timeline. Neuralink won first‑in‑human approval in May 2023 and implanted multiple patients under PRIME. Synchron completed the first U.S. endovascular implant during a July 2022 early feasibility study. Precision Neuroscience earned 510(k) clearance in April 2025 for its Layer 7 ECoG system.
Coverage questions: payers, benefits design, and ongoing maintenance
Reimbursement remains unsettled. Ask who will cover surgery, implants in brain tissue or skull access, device replacements, and long‑term maintenance for stroke or spinal cord indications.
- Confirm study evidence and timelines from the company.
- Request documentation and required training for clinical staff.
- Talk early with payers and TPAs about coverage for eligible patients.
“Regulatory status shapes clinical partnerships, costs, and whether a pilot can scale.”
Case studies and breakthroughs moving BCIs into the present
Concrete trials now show how decoding real brain signals turns imagined actions into fast, usable control. You can use these examples to set realistic goals for pilots and measure progress against proven benchmarks.
Speech decoding and “mindwriting” benchmarks
Leading studies give clear numbers you can trust. A Stanford study decoded imagined handwriting at about 86 characters per minute. UCSF’s high-density ECoG work produced intended speech and facial expression outputs near 78 words per minute.
BrainGate trials have shown thought-controlled typing at roughly 90 characters per minute. These studies show that communication speed is now within reach for many patient workflows and accessibility pilots.
Thought-controlled cursors, robotic limbs, and real-world autonomy
Animal studies paved the way: monkeys led early movement control work, and later patients translated that into robotic-arm demos and cursor control for everyday tasks.
Endovascular devices like Synchron’s Stentrode enable thought-driven clicks and typing for people with paralysis. That movement from lab to clinic shows how device choice, electrodes, and placement shape performance.
- Benchmarks: use study speeds to set words-per-minute and characters-per-minute targets.
- Training: expect calibration and weeks of practice for reliable control.
- Hardware: count channels and electrode type when you compare devices for pilot use.
- Reliability: measure error rates to pick suitable workflows like messaging or basic navigation.
“These examples show real autonomy gains—sending messages, navigating apps, and reducing caregiver load.”
Technical challenges and active research fronts
Practical tradeoffs in signal quality, durability, and AI decoding define current research priorities. You need clear facts to choose the right approach for pilots and long-term deployment.
Signal quality vs. accessibility: invasive and non-invasive tradeoffs
High-fidelity electrodes in brain tissue give the best control, but they require surgery and raise risk. Non‑invasive methods are safer and easier to roll out, yet they capture weaker signals and more noise.
Surface approaches like ECoG often hit a middle ground: better decoding than scalp EEG without penetrating tissue. New work at Johns Hopkins that senses tiny tissue deformation through the skull shows promise for higher resolution without surgery.
Durability, the “butcher ratio,” and biocompatibility
The so‑called butcher ratio highlights how penetrating arrays can damage many neurons per useful channel. That limits scaling across larger brains and long-term implants.
Manufacturers now focus on flexible threads, improved coatings, and softer materials to reduce encapsulation and signal drift. Even so, questions remain about lifetime, replacement strategies, and chronic safety during widespread development.
AI advancements: faster, safer, and more accurate decoding
AI models are improving feature extraction, adaptive filtering, and closed‑loop feedback. That boosts speed and stability across modalities and reduces the need for repeated recalibration.
Still, the development pipeline faces practical hurdles: reproducible manufacturing, wireless reliability, battery safety, and regulatory evidence for long‑term use.
- Tradeoffs: choose a method that fits your performance and risk tolerance.
- Durability: expect maintenance plans and replacement timelines for implants.
- AI: leverage adaptive models to stabilize real‑world control.
- Near term: ECoG and improved non‑invasive methods will broaden access in 12–24 months.
“Signal quality, materials, and smarter decoding will determine which approaches scale safely.”
Market outlook: Adoption curves, vendors, and investment signals
The market is waking up fast — and the next few years will sort early pilots from lasting workplace tools.
Market size and funding: the sector is forecast to grow from nearly $2B in 2023 to about $6.2B by 2030. Major company funding signals matter: Neuralink has raised over $1B, Synchron has $100M+ and partnerships with Nvidia and Apple, and Precision Neuroscience earned 510(k) clearance in 2025. These moves show shifting priorities from research to commercial development.
Layered adoption curve: expect accessibility pilots and monitoring applications to lead now. Over time, higher-bandwidth devices and clinical-grade implants will expand into richer applications like speech decoding and advanced control.
- Practical timeline: pilots today, selective commercial rollouts in 2–4 years, broader adoption as regulation and support mature.
- Vendor signals: funding, partnerships, and clear roadmaps indicate product readiness and supportability.
- Procurement view: headsets for near-term ROI; implants and high-fidelity devices as strategic investments.
People and change management will shape adoption as much as technology. Train users early, track simple metrics, and require vendor transparency on study results, security, and maintenance.
“Track funding, regulatory milestones, and independent studies — they tell you which devices are ready for your workplace.”
Simple framework to watch:
- Funding & partnerships
- Regulatory milestones and study outcomes
- Vendor transparency on security and roadmaps
- User adoption, support readiness, and time-to-value
BCI vendor evaluation checklist for enterprises
When you evaluate vendors, focus first on how devices balance practical safety with signal quality for your users. This keeps procurement tied to outcomes, not specs alone.
Safety profile, signal fidelity, and data controls
Compare vendor claims across electrode type, channel count, and placement (EEG, ECoG, endovascular, intracortical). Those choices shape both safety and decoding performance.
Demand clinical evidence: FDA designations, peer‑reviewed studies, and real‑world outcomes. Check how the company logs consent, encrypts data, and supports audit trails.
“High channel counts can improve control but may raise surgical and maintenance risk.”
Integration, support, and total cost of ownership
Assess wireless stacks, battery life, APIs, and OS compatibility so IT work is predictable. Ask about SLAs, on‑site service, training, and parts availability.
- Map total cost: hardware, accessories, software licenses, and staff time.
- Scrutinize roadmaps and replacement cycles to avoid locked platforms.
- Structure pilots and contracts with clear success metrics and shared risk.
Conclusion
This conclusion lays out clear next steps so you can move from curiosity to a focused pilot that delivers measurable value.
Modern brain-computer interfaces span non-invasive headsets to ECoG and endovascular implants. Clinical studies now show speech decoding, handwriting-to-text, and thought-based computer control. Vendors such as Neuralink, Synchron, and Precision Neuroscience signal fast progress, while consumer gear from Neurable highlights fatigue and focus insights.
Practical next moves: start small, pick clear applications, use the vendor checklist we provided, and pair pilots with strong change management. Build a multi-year roadmap that matches growing intelligence and comfort with real workplace needs.
Ready to act? Choose one focused pilot, measure impact, and scale what works—then explore AR/VR workspaces via AR/VR workspaces for next-level use.





